Keywords
non-invasive ventilation
prone positioning
severe acute respiratory distress syndrome Coronavirus-2
Abstract
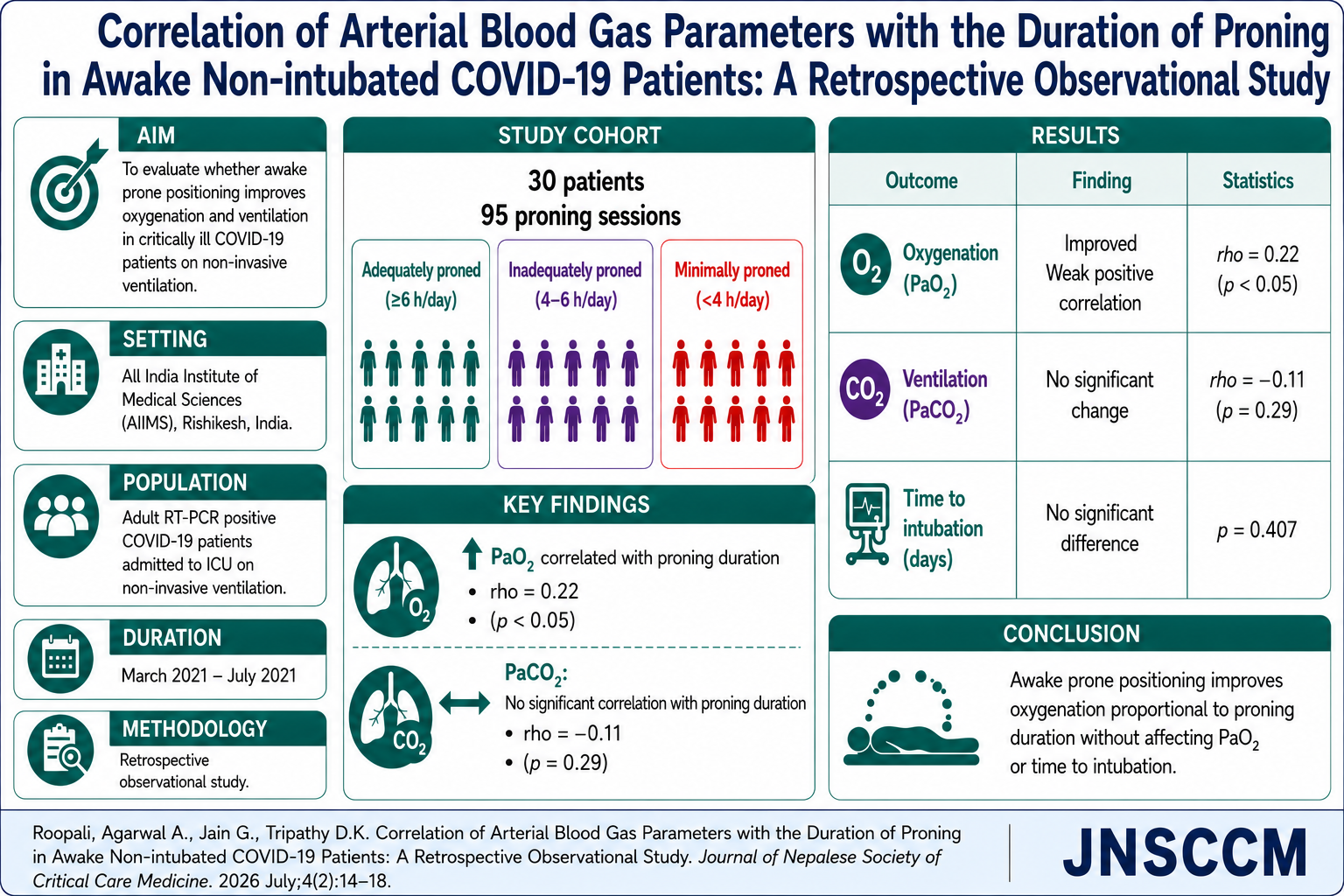
Background and aims: Prone positioning (PP), which has been known for decades to increase oxygenation in mechanically ventilated patients with moderate to severe acute respiratory distress syndrome (ARDS), was also practiced in Coronavirus disease (COVID-19) patients. We hypothesized that prone positioning in critically ill COVID-19 patients would improve oxygenation and ventilation and potentially translate into improved survival.
Methods: A retrospective, observational study was conducted in All India Institute of Medical Sciences, Rishikesh, from March 2021 to July 2021. SARS-CoV-2 reverse transcriptase – polymerase chain reaction (RT-PCR) positive adult patients admitted to the ICU on non-invasive ventilation were included in the study. Proning durations were categorised as adequately proned (at least six hours/day), inadequately proned (four to six hours/ day) and minimally proned (less than four hours/ day).
Results: The 30 included patients underwent 95 proning sessions. The change in PaCO2 had no statistically significant correlation with the duration of proning in hours (rho= -0.11, p = 0.295). There was a statistically significant weak positive correlation between the change in PaO and duration of proning in hours (rho = 0.22, p<0.05). For each hour of proning, percent increase in PaO2 was by 0.44 percent. There was no significant difference between the groups in terms of time to intubation (days) (p = 0.407).
Conclusion: This study demonstrated that prone positioning in awake, non-intubated COVID-19 patients with acute respiratory failure improves oxygenation proportional to proning duration without affecting PaCO2 levels.
References
WHO. Naming the coronavirus disease (COVID-19) and the virus that causes it: https://www.who.int/ emergencies/diseases/novel-coronavirus-2019/ technical-guidance/ Accessed April 16, 2020
Gattinoni L, Taccone P, Carlesso E, Marini JJ. Prone position in acute respiratory distress syndrome: rationale, indications, and limits. Am J Respir Crit Care Med. 2013;188(11):1286–93.
Ali HS, Kamble M. Prone positioning in ARDS: physiology, evidence and challenges. Qatar Med J. 2019;2019(2):14.
Weiss TT, Cerda F, Scott JB, et al. Prone positioning for patients intubated for severe acute respiratory distress syndrome (ARDS) secondary to COVID-19: a retrospective observational cohort study. Br J Anaesth. 2021;126(1):48–55.
Beheshti A, Pakzad R, Goudarzi Rad M, Abdi F, Zaheri F, Mirzadeh N. Effect of prone position on respiratory parameters, intubation and death rate in COVID-19 patients: systematic review and meta-analysis. Sci Rep. 2021;11(1):14407.
Gattinoni L, Tognoni G, Pesenti A, et al. Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med. 2001;345(8):568–73.
Berrill M. Evaluation of oxygenation in 129 proning sessions in 34 mechanically ventilated COVID-19 patients. J Intensive Care Med. 2021;36(2):229–32.
Scaravilli V, Grasselli G, Castagna L, et al. Prone positioning improves oxygenation in spontaneously breathing nonintubated patients with hypoxemic acute respiratory failure: a retrospective study. J Crit Care. 2015;30(6):1390–4.
Weatherald J, Solverson K, Zuege DJ, Loroff N, Fiest KM, Parhar KK. Awake prone positioning for COVID-19 hypoxemic respiratory failure: a rapid review. J Crit Care. 2021;61:63–70.

This work is licensed under a Creative Commons Attribution 4.0 International License.